Skip to content
About Dry Eyes Disease
Symptoms & Causes
Dry Eye Center
Resources
Blog
Patient Education Videos
Brochures
X
Dry Eye Assessment Test
Home
»
Dry Eye Assessment Test
Personal Info
Name
Age
Gender:
Gender
Male
Female
Other
Mobile number
City
Start Survey
Have you experienced any of the following during the last week:
All of the time
Most of the time
Half of the time
Some of the time
None of the time
Eyes that are sensitive to light?
4
3
2
1
0
Eyes that are feel gritty?
4
3
2
1
0
Painful or sore eyes?
4
3
2
1
0
Blurred Vision?
4
3
2
1
0
Poor Vision?
4
3
2
1
0
Subtotal score for answers 1 to 5
0
Have problems with your eyes limited you in performing any of the following during the last week:
All of the time
Most of the time
Half of the time
Some of the time
None of the time
Reading?
4
3
2
1
0
Driving at night?
4
3
2
1
0
Working with a computer or bank machine(ATM)?
4
3
2
1
0
Watching TV?
4
3
2
1
0
No Answer
N/A
N/A
N/A
N/A
Subtotal score for answers 6 to 9
0
Have your eyes felt uncomfortable in any of the following situations during the last week:
All of the time
Most of the time
Half of the time
Some of the time
None of the time
Windy Conditions?
4
3
2
1
0
Places or areas with low humidity (very dry)?
4
3
2
1
0
Areas that are air conditioned?
4
3
2
1
0
No Answer
N/A
N/A
N/A
Subtotal score for answers 10 to 12
0
Submit Your Answers
Your Score is
0
You Should consult Dry Eye Specialist
Visit our Dry Eye Center of Excellence and consult Dry Eye specialist
For more details:
+91 90008 52020
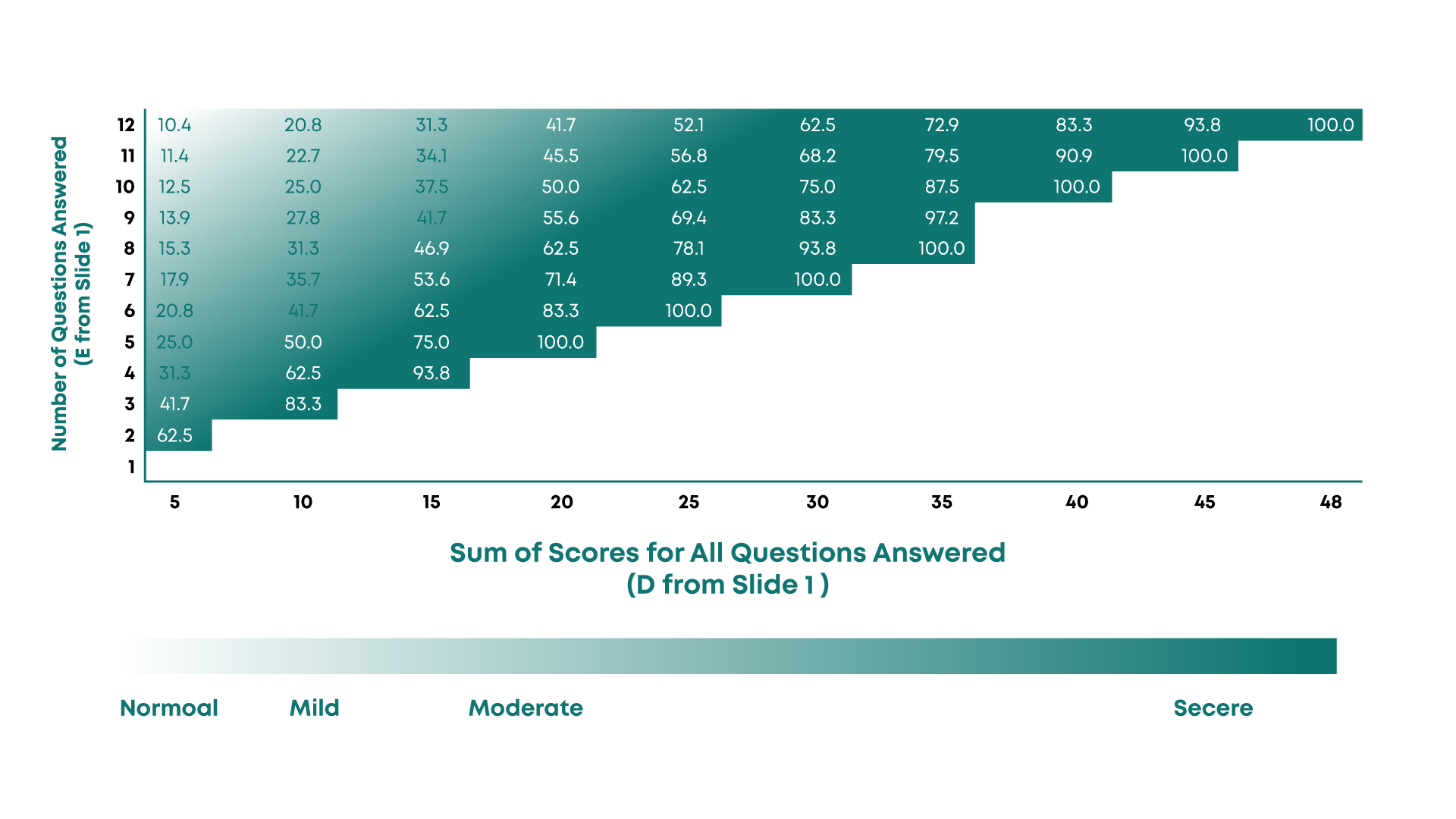
0 - 10
:
Normal
11 - 30 : Mild
31 - 50 : Moderate
51 - 100 : Severe
Name
Age
Gender
Mobile Number
City / Place
------------
Have you experienced any of the following during the last week:
Eyes that are sensitive to light?
Eyes that are feel gritty?
Painful or sore eyes?
Blurred Vision?
Poor Vision?
Subtotal Score for answers 1-5
------------
Have problems with your eyes limited you in performing any of the following during the last week:
Reading?
Driving at night?
Working with a computer or bank machine(ATM)?
Watching TV?
Subtotal Score for answers 6-9
------------
Have your eyes felt uncomfortable in any of the following situations during the last week:
Windy Conditions?
Places or areas with low humidity (very dry)?
Areas that are air conditioned?
Subtotal Score for answers 10-12
------------
Total Score
Send
Facebook
Instagram
Linkedin
Youtube
Phone: +91 90008 52020
About Dry Eye Disease
Symptoms & Causes
Patient Education Videos
Ask an Expert
Find a Clinic
Ocular Surface Disease Index (OSDI)
General Quiz
Employee Quiz
Student Quiz
Copyright © 2025
BlinkBreak
| Powered by Pristine Eye Hospitals